
In this essay we will discuss about Disaster and its Management. After reading this essay you will learn about:- 1. Introduction to Disaster 2. Types of Disasters 3. Triage 4. Disasters and Health 5. Disaster Prone Areas 6. Examples 7. Consequences 8. Warning System 9. Management 10. Casualties.
Essay on Disaster and Its Management
Essay Contents:
- Essay on Introduction to Disaster
- Essay on the Types of Disasters
- Essay on the Triage of Disaster
- Essay on Disasters and Health
- Essay on Disaster-Prone Areas
- Essay on the Examples of Some Disasters
- Essay on the Consequences of Disaster
- Essay on Disaster Warning System
- Essay on the Management of Natural Disaster
- Essay on the Casualties for Disaster
1. Essay on Introduction to Disaster:
A disaster gives rise to mass casualties—a large number of wounded and dead—within a short span of time. It also results in temporary disruption of the existing medical service which find it extremely difficult to cope up with the sudden rush of mass casualties due to paucity of time, technical manpower and the resources at their command.
Under such a situation, the medical ethics calls for resort to the principle of ‘triage’ in handling the mass casualties which aims at provision of “maximum benefit to the greatest number” in the face of such constraints.
The word ‘triage’ simply means “the action of assorting according to quality”. The principles of ‘triage’ in handling of mass casualties have been effectively followed by the military medical services during the previous two World Wars.
The dictionary meaning of ‘disaster’ is a calamity, a sudden or great misfortune. However, unlike a calamity or misfortune affecting an individual or a family, a disaster occurs like an explosive epidemic affecting masses and usually culminates into undue loss of life and/or property. It is always associated with mass panic and usually large scale movement of population.
It disrupts the normal social life and administrative organization of the affected community and imposes a sudden demand on the public health machinery to cope with this stressful situation for which it is not usually fully prepared. The consequence of such unpreparedness is reflected by an increase in the amount of morbidity, mortality and disability which the community suffers.
2. Essay on the Types of Disasters:
From the point of view of their impact on health, disasters can be broadly put into four categories:
(i) Earthquakes
(ii) Cyclones and other destructive winds,
(iii) Floods and sea surges and
(iv) Other inundations.
According to their genesis, the disasters can also be classified into two broad categories, viz.:
(a) Natural, such as earthquakes, volcanic eruptions, floods, etc. and
(b) Man-made which can be further divided into:
(i) Intentional e.g., dropping of atom bombs on Hiroshima and Nagasaki and
(ii) Unintentional but usually due to human negligence as in case of Bhopal gas tragedy and the Chernobyl disaster.
From the point of view of protection of disabled people, disasters can be again categorized as:
(i) Those with no warning period and
(ii) Those with a warning period which permits evacuation of people at risk to safe places of shelter.
3. Essay on the Triage of Disaster:
Ideally, a two-stage triage’ operation has been advocated to handle the mass casualties resulting from disaster. This should be instituted as expeditiously as possible soon after the disaster at two levels i.e., at the scene of the disaster and casualty receiving area of the hospital.
Triage at the Disaster Site:
The technical manpower (medical and paramedical) details at the scene of disaster must appreciate that the prime goal of triage is to reduce” the overall loss of life and limb. The triage teamour triageur is provided with necessary first-aid and resuscitative equipment to achieve this goal. The triage process ensures that the patients most in need of hospital capability are evaluated first.
They are allotted priority for treatment and evaluation to the hospital as under:
First Priority:
These are casualties with conditions which represent a direct threat to life and require immediate corrective measures/resuscitation e.g., airway obstruction, external haemorrhage, shock etc. These casualties are considered for evacuation to hospital as soon as their condition becomes stabilized.
Second Priority:
These are casualties with injuries that could lead to death if not treated promptly but are not immediately life—threatening as first priority injuries e.g:
(a) Penetrating or open injuries of the abdomen,
(b) Major bums,
(c) Closed head injuries with deteriorating consciousness and
(d) Vascular injuries needing repair when haemorrhage has been controlled.
Third Priority:
These are casualties which need hospitalization but are not in urgent need of it.
Their evacuation to the hospital can be delayed even up to several hours without any serious threat to their life e.g:
(a) Moderate burns,
(b) Fractures and dislocations,
(c) Eye injuries,
(d) Lacerations requiring debridement and surgical repair and
(e) Facial injuries not interfering with the airway.
Minor Injuries:
Besides casualties falling into above mentioned three categories, there may be a large number of cases with minor injuries e.g., abrasions, contusions, foreign bodies embedded in skin, small lacerations, sprains and strains.
Such cases should be encouraged to help treating each other and moved to a site away from the main disaster areas so that the triage effort in respect or more serious casualties does not get adversely affected.
Dead and Hopelessly Wounded:
While dead only need to be properly covered and removed to a place outside the triage area from where their identification could be made, the hopelessly wounded, moribund cases needing difficult, complicated and time—consuming care with little chances of survival after surgery, should be sent outside the triage area where they can be kept comfortably and wait until medical personnel have time to attend to them.
4. Essay on Disasters and Health:
Disasters can be classified into two broad categories viz. Natural disasters, such as earthquakes, volcanic eruptions, floods etc. and man-made disasters which may be intentional (dropping of atom bombs as in the case of Hiroshima and Nagasaki, etc.) and unintentional (like Bhopal Gas Tragedy and Chernobyl Disaster).
“Disasters are not a new phenomenon in the ecology of man. What is new is the increasing awareness that some kind of disaster management should be promoted. It has become clear that improvisation is not the effective approach in a critical and emotive disaster situation. Pre-disaster planning and preparedness has become the order of the day and disaster epidemiology an integral part of a multidisciplinary approach to disaster”.
5. Essay on Disaster-Prone Areas:
These can be classified into:
(A) Natural high-risk areas, such as:
(i) Seismically active or earthquake—prone areas,
(ii) River flood plains,
(iii) Tidal wave flood plains,
(iv) Areas subject to tropical storms and
(v) Areas in the vicinity of active volcanoes.
(B) Potential man-made hazardous areas will include:
(i) Down of a dam,
(ii) Sites beneath which mining has taken place,
(iii) Sites in the vicinity of industrial plants with explosion/pollution risk,
(iv) Sites in the shadow of industrial refuse pits and
(v) Areas near major airports.
6. Essay on the Examples of Some Disasters:
A few examples of disasters which are still fresh in the memory of living generations are:
(A) Atom Bombing of Hiroshima (6 August 1945) and Nagasaki (9 August 1945) during the Second World War is regarded as the worst man-made disaster of the century with estimated casualties of 1, 20,000 and 75,000, respectively.
(B) Guatemala Earthquake (1976) in which 92% lost their homes, about 76,000 sustained injuries and some 23,000 got killed.
A small survey of victims of this disaster brought out such startling findings as:
I. —84% of the victims had no social security in the form of insurance.
II. —46% were dissatisfied with the medical care received by them.
III. —13% could not return to their former employment because of their injuries, i.e., they needed vocational rehabilitation.
IV. —12% had to wait 2-3 days and 16% for one week before admission into a hospital.
V. —Even for first-aid, 13% had to wait for 2- 4 hours, 12% for 4-8 hours and 21% for 2- 3 days.
(C) The Tidal Wave and Cyclone Disaster in Andhra Pradesh (1977) which claimed some 25,000 lives. The victims included mainly the young people, the old and the weak.
(D) Bhopal Gas Tragedy (1988) is regarded as the worst air pollution disaster so far and was due to accidental- leakage of methyl isocynate (MIC) from its plant. It affected about two lakh people and claimed 1,754 lives, according to one published report.
(E) Chernobyl Nuclear Plant Disaster (1986) which resulted in the death of 28 people and 203 suffered from radiation sickness. The material losses amounted to two billion roubles approximately.
7. Essay on the Consequences of Disaster:
The consequences and their magnitude primarily depend upon the nature of the disaster itself. Some of these are predictable qualitatively, if not quantitatively.
These can be put into two broad categories:
(A) Human suffering due to lack of shelter, injury, disability and death.
(B) Monetary loss due to loss of property individual and public.
The health effects and other effects of a natural disaster can also be categorized into ‘short-term’ and ‘long-term’ effects. Short-term effect vary according to the nature of the disaster.
For example:
(a) In earthquakes many deaths occur. Severe injuries requiring intensive medical care are over-whelming. Falling roofs and walls while standing up ire common cause of fractured clavicles. Spinal injuries and pelvic fractures are also common. Food scarcity and population movements are rare but increased risk of infection due to exposure by shelter-less victims remains a potential problem.
(b) During high winds, few deaths occur. Some injuries moderate. Food scarcity is commonly seen and population movements are rare. Hurricanes usually leave behind a significant number of persons with physical disabilities such as spinal cord lesions blindness and deafness.
(c) During tidal wave and flash floods, many deaths occur although severe injuries are few. Food scarcity and population movements are common. Potential increased risk of infections is present.
(d) During floods, deaths and severe injuries are few. Food scarcity and population movements are common. Potential risk of infectious diseases is always present.
Besides above, the victims of any disaster are also prone to suffer from a variety of psychological disorders, such as, (i) various forms of anxiety, depression in predisposed individuals, (ii) Post- disaster syndrome (temporary confusion, disorientation).
Increased risk of communicable diseases remains a potential risk following natural disasters which result into overcrowding and deterioration in environment hygiene, particularly affecting the water supply and disposal of human wastes. This again depends largely on the previous sanitary levels of the area. Sometimes shortage rather than contamination of water supply emerges as a major problem.
During the famines, prolonged malnutrition predisposes to gastroenteritis, measles and respiratory group of infections which become leading causes of death. Disasters also disrupt the ongoing diseases control programmes in that area.
Explosive outbreaks of malaria (more than 75,000 cases) occurred after Flora hurricane across Haiti in 1963 which destroyed houses sprayed with DDT and also increased the breeding sites of in seeds. Besides the above problems, burial cremation of corpses and disposal of car-cases are other major problems to be tackled with on a war-footing.
8. Essay on Disaster Warning System:
Coastal regions of India are vulnerable to the cyclonic storms. These are extremely destructive systems and frequent the Indian subcontinent during April-May and October-December every year.
(i) Cyclone Warning System:
The Indian Meteorological Department (IMD) is well-equipped for tracking the cyclonic storms and their intensity and warning the public about their land-fall. The IMD is equipped with cyclone tracking radars at Karaikal, Chennai, Machili-patnam, Visakhapatnam, Paradeep and Kolkata on the east coast as well as at Goa, Mumbai and Bhuj on the West Coast.
(ii) Insat Disaster Warning System (DWS):
Indian National Satellite (INSAT). In this system, called the Disaster Warning System (DWS), the warning message which is originated at Cyclone Warning Center is transmitted to the satellite which, in turn, broadcasts it for instantaneous reception by receiving sets wherever they are deployed.
By a system of selective addressing, warnings are received by only those receivers for whom the warning is intended. The selective addressing is done by first transmitting a digital code which is followed by the actual warning message in the local language.
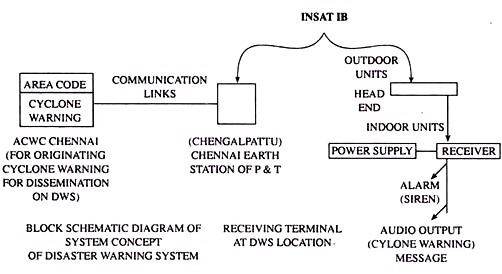
(iii) Brief Technical Description of the (DWS) System:
Block Schematic Diagram of the system concept of the DWS is given below. The DWS used the INSAT TV Transponder for the transmission of the warnings. At the originating stations, i.e., ACWC Chennai, the areas code of the places to which the warnings are to be transmitted is sent through a specially designed code generator to the Chengalpattu earth station of the Department of Telecommunication. These signals, sent to INSAT in the 6 GHz band, are received by all the DWS receivers in the 2.5 GHz band.
9. Essay on the Management of Natural Disaster:
A common man has to play a very distinctive and decisive role when residing in a natural disaster prone area. During pre-disaster phase, he is mainly concerned with his disaster pre- preparedness with a view to reduce physical injuries, subsequent disability/mortality.
During the active disaster phase itself, his main role is to ensure maximum safety for himself and his family members and during the post-disaster phase to curtail its after-effects, such as, prevention of his own illness and that of his family members and outbreaks of epidemics in the community. He also strives for early rehabilitation during this phase.
“Nothing in life is to be feared,
It is only to be understood”.
—Marie Curie
There is a wrong notion in the minds of many that natural disaster management is the sole responsibility government, international agencies and voluntary organisations; the common man is only a victim of such calamities and incapable of playing any major role in preventing or mitigating the sufferings caused by various natural disasters such as earthquakes, floods, droughts, cyclones, volcanic eruptions etc.
But comprising of common men, can certainly play an active role by taking certain timely steps before, during and following the occurrence of a natural disaster.
These steps aim at:
(a) A good state of preparedness to reduce its impact.
(b) To ensure timely first-aid and life saving resuscitative measures through proper training to prevent disablement and mortality, till such time the expert medical aid is not available, and
(c) Better handling of problems of health, hygiene, sanitation and outbreaks of epidemics which normally follow in the wake of a natural disaster.
(i) During Pre-Disaster Phase:
This is the time when a common man should strive to increase his disaster awareness through mass media such as available literature, newspaper reports, radio/television programme etc., and by listening to lectures, group discussions, seminars, etc., on this subject. He should apprise himself of whether the area where he works/lives/visits, is exposed to potential risks of any natural disaster.
If ‘yes’ then what are the risks involved and how these can be prevented or mitigated in terms of consequent morbidity, mortality and disablement. Such awareness and prior knowledge will prove to be an asset, a basis for his confidence in self-help and moral support when-ever confronted with such calamity irrespective of the fact whether it occurs with prior warning (e.g., earthquakes).
In case he receives a prior warning then he should promptly communicate it to all family members and neighbours to promote man residing in a disaster prone area voluntarily comes forward to receive training in various life- saving measures and first-aid whenever training courses are arranged for the general public.
Every individual in possession of such training must impart it to others, particularly his family members and neighbours as his individual contribution, towards community preparedness in facing the disaster with self-confidence without any panic even if the organised medical help/rescue teams arrive late due to some unavoidable reasons.
In disaster-prone areas, the training in disaster preparedness activities is usually arranged by local administrative/health authorities and voluntary health organisations, etc., for various population groups in schools, colleges, factories and various other work places as per their conveniences so as to attract the maximum voluntary response.
The training normally caters for:
1. Training in first-aid in case of injury, haemorrhage, burns, drowning, snake-bite, etc.,
2. Training in life saving resuscitative measures when expert medical help is not available, e.g., clearing the obstructed airway, artificial respiration, external cardiac massage, etc.
3. Training in rescue of disaster victims and their transportation to a treatment centre hospital.
4. Training in basics of hygiene and sanitation as relevant to a disaster situation.
(ii) Hygiene and Sanitation:
The training in hygiene and sanitation is of particular importance to a common man as it enables him to take suitable steps to prevent post- disaster morbidity and mortality due to outbreaks of epidemic.
The training mainly focuses upon:
1. Procurement of drinking water from authorised, safe sources.
2. Disinfection of drinking water at source/consumer’s end.
3. Avoiding open air defecation.
4. Proper disposal of all types of solid and liquid wastes.
5. Antifly, antirodent and other vector control measures.
6. Environmental hygiene and sanitation.
7. Personal hygiene.
8. Avoidance of overcrowding.
9. Measures against lice infestation, scabies, etc.
Every common man must maintain an uptodate record of his immunisation status in respect of self and every family member. The record-card should also contain information on blood group, allergies, hypersensitivity to drugs, etc., for the convenience of the medical authorities.
(iii) During Disaster (Active Phase):
A common man should develop courage and boldly face the unavoidable situation. He should avoid developing signs of fear get panicky, remain calm and provide moral support to his family members. When inside a crowded and enclosed space (cinema hall, auditorium, temple, church, etc.) panic must be avoided, otherwise it leads to stampede.
(a) Do not trample over ruins to avoid injury to those trapped underneath.
(b) Do not remove rubble unless absolutely sure that it will not further cause collapse of the building. Manual removal should be preferred using spades and picks gently and cautiously.
(c) Ensure easy availability of essential items required for rescue work in the house/neighbourhood e.g., ladders, ropes, spades, picks, heavy gloves, pocket torches, etc.
(d) Make all out efforts to locate those under the rubble by ensuring absolute silence of first and then calling them loudly from different points in the ruins or by knocking on pieces of metal pushed down into the rubble or by using loudspeaker when available.
(e) On recovery, the victim must be immediately provided with essential first-aid and moral support and shifted to the nearest place where medical facilities are available. If a stretcher is not available then one can be improvised using large wooden planks, doors, ladders, bamboos, camp beds, blankets, thick bed sheets and plastic sheet, etc.
(f) Observe maximum precaution while lifting an injured person. Ensure that his head neck and trunk remain in the same axis otherwise it may aggravate certain injuries e.g., spinal injury.
Avoid jerks while transferring the casualty and ensure that the stretcher must go forward with the patient’s head foremost, prevent his exposure to cold by covering him with a blanket. However, every effort should be made to obtain the services of proper rescue teams.
Maximum casualties occur during this active phase.
The well known risk factors should be avoided by observing following precautions:
(a) Immediately switch off the main electric switch to prevent risk of electrocution. After the damage use torch if required.
(b) Immediately extinguish gas stove and other sources of fire- to prevent fire hazards.
(c) Immediately close the running water tap/main pipe line to prevent water logging/flooding of the area due to its damage.
(d) Do not come out on a narrow street-lane with tall buildings on its side during an earthquake. If an open ground or a wide street/open square free from the risk of falling building is not available nearby, it is more secure to get under a door way or into an inside corner of a room or under a table under such circumstances.
If the house is concrete of steel and on the ground floor then it is safer to come out and walk along the middle of the street towards and square. If on a higher floor ten it is safer to remain indoors near on internal pillar. However, if the house is build of stone, brick or similar material and located above the ground floor then avoid going into the stair wells and take position under a doorway in a load- bearing well.
(e) Do not remain outdoor in open areas during cyclones and hurricanes to avoid injury from flying objects of various kinds. Better get confined inside wind proof pucca house.
(f) Do not touch electric poles, fallen electric wires, etc. to avoid accidental electrocution.
(iv) Post-Disaster Phase:
This is the phase of recovery from psychological, physical and material damage caused by the disaster. A common man must install confidence in himself and his family members to facilitate gradual switch over to previous normal routine of life. For early rehabilitation, he should take advantage of all post disaster relief services offered by the government and other agencies.
He should however take following precautions during this phase:
(A) If he has been sent to a place of temporary shelter, he and all members of his family must observe religiously the various preventive measures advised by the health authorities such as:
(a) Not to resort to open air defecation, use trench or other types of sanitary latrines provided for
(b) Obtain drinking water from authorised sources only/use bleaching powder or chlorine tablets or boil it as per facilities available,
(c) Ensure proper disposal of all types of waste,
(d) Observe antifly, other vector control and rodent control measures,
(e) Ensure personal hygiene and food hygiene and
(f) Ensure proper ventilation of accommodation provided for a follow “head to foot” sleeping arrangement as practiced in army when overcrowding is not avoidable.
(B) The individual must report promptly in case he himself or a member of his family falls sick. He should ensure a thorough medical check-up of those family members who fall under the category of “vulnerable groups” e.g., physically and mentally retarded, disabled, infants (particularly those not breasted), children, pregnant women, nursing mothers and those chronically ill.
(C) Before leaving the temporary shelter and moving into his own house the individual must ensure that all necessary repairs have been carried out in respect of damage done by the disaster and the house has been declared fit for human occupation by the authorities concerned, both from safety and hygiene and sanitation point of view.
10
. Essay on the Casualties for Disaster:
This includes rescue of the injured and those trapped in wreckage etc., first aid, evacuation to hospitals and definitive treatment.
The efficiency of management depends upon:
(i) Availability of enough medical and paramedical personnel trained in disaster medicine,
(ii) Adequate hospital facilities to care for victims,
(iii) Enough transport (ambulances, helicopters, etc.) for speedy evacuation of casualties and
(iv) Standing orders/written plans for individual hospital and all other agencies likely to get involved in providing relief to disaster victims.
Handling of Casualties:
When the number of casualties is high and the medical facilities are inadequate, the concept of ‘triage’ or classification of patients according to the priority in receiving the medical attention (as in case of war) is followed so that the maximum number of injured are benefitted despite a very short period of medical attention (sometimes as little as two or three minutes for each patient).
For example, the casualties can be allotted the priorities as:
a. Priority I- Those who have problems with vital functions (respiratory, circulatory etc. and unconscious patients) and need immediate treatment.
b. Priority II- Seriously injured who require an urgent operation but can wait for 6-12 hours after receiving the medical first aid.
c. Priority III- Hopeless cases whose sufferings must be relieved as much by a treatment as by spiritual comfort.
All other cases with slight injuries can be called priority IV cases (last priority) who should be separated from other priority groups to prevent psychic disorders in them which precipitate panic and chaos.
Recommendations for Effective Management:
For tackling the problems associated with disasters more effectively recommendations on following aspects have been made:
(a) More attention towards public awareness and preparedness.
(b) Publishing information through public media (pamphlets, posters, radio, TV etc.)
(c) Special training to medical, para-medical. Red Cross and other voluntary workers (teachers, students, NCC, scouts etc.)
(d) Special training to disabled high risk category so that they now how to protect themselves against fumes, gases and other containments.
(e) What action to be taken in case of fire, bums, haemorrhage, fractures etc.?
(f) How to breathe when there is little oxygen available?
(g) How to survive when buried under rubble, an avalanche or other heavy objects?
(h) Dissemination of information regarding location of main fuse box, main water valve, gas tap and fire extinguisher and also where candles, matchbox, wheel chair and crutches are kept.
(i) How to use the emergency bag containing essential items which should be provided to every disabled person according to nature of his/her disability?
(j) Suitable and adequate transport for speedy evacuation of disaster victims to hospitals,
(k) Special plans for emergency expansion of hospital facilities, e.g., extra beds, surgical facilities, transfusion fluids, drugs, patients’ clothing, food, water, fuel, medical comforts, stand-by generators etc.
(l) Plans for opening emergency/auxiliary treatment centres and rehabilitation centers for disabled people,
(m) Every country to have Manual of Disaster Preparedness and its own relief plans,
(n) Courses in management of disaster injuries and other associated health problems to be included in the medical curriculum,
(o) Attention to building location and construction standards,
(p) Provision of hazard-warning systems,
(q) Insurance (social security) of people residing in disaster-prone areas,
(r) Measures to mitigate a future disaster,
(s) Pre-disaster planning which means the general organisation required to promote the greatest possible efficiency in disaster management at the lowest cost. In further implies a reliable assessment of urgent and long-term needs in terms of mass casualty management.